

QoL, CIs, QALYs, and Individualized Rehabilitation: The Clinical and Practical Benefits of Regularly Assessing the Quality of Life of Adult Cochlear Implant Recipients
 , , ,
, , ,  , , , , , , , , , ,
, , , , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Assessments and Intervals
2.2.1. Generic QoL
2.2.2. Disease-Specific QoL
2.3. Bias
2.4. Statistics
3. Results
3.1. Participants
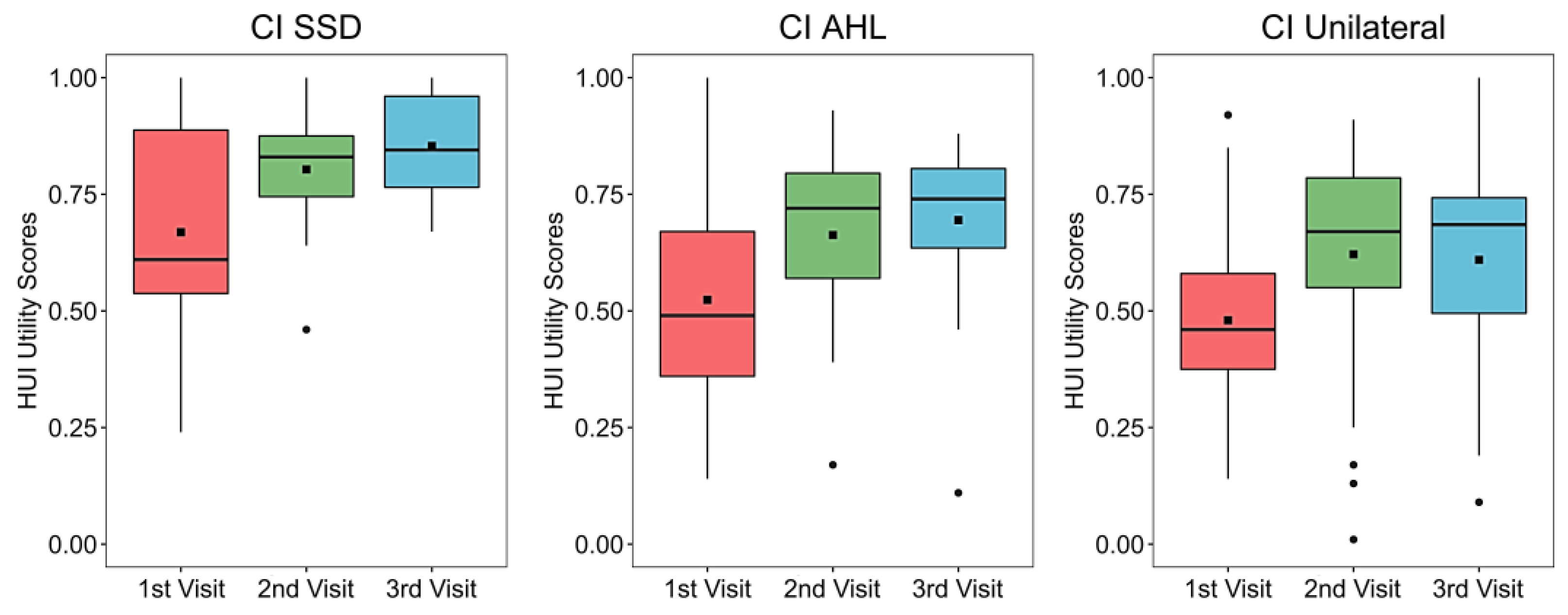
3.2. Generic QoL
3.3. Disease-Specific QoL
3.3.1. SSQ12
3.3.2. NCIQ
3.4. Audio Processor Daily Use
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SSD | AHL | Unilateral | |
|---|---|---|---|
| Cochlear implant | |||
| SONATATI | 8 | 10 | 15 |
| SYNCHRONY | 7 | 7 | 6 |
| SYNCHRONY PIN | 0 | 5 | 15 |
| CONCERTO | 1 | 2 | 9 |
| CONCERTO PIN | 1 | 1 | 2 |
| Missing | 0 | 1 | 11 |
| Total | 17 | 26 | 58 |
| Audio processor | |||
| SONNET | 12 | 17 | 39 |
| RONDO | 4 | 2 | 8 |
| OPUS 2 | 0 | 3 | 5 |
| Missing | 1 | 4 | 6 |
| Total | 17 | 26 | 58 |
| Electrode array | |||
| FLEX28 | 8 | 13 | 30 |
| FLEX24 | 4 | 6 | 9 |
| FLEX20 | 1 | 2 | 1 |
| FLEXSOFT | 0 | 1 | 0 |
| MEDIUM | 0 | 1 | 0 |
| COMPRESSED | 0 | 1 | 3 |
| STANDARD | 4 | 1 | 4 |
| Missing | 0 | 1 | 11 |
| Total | 17 | 26 | 58 |
| n | Visit 1 | n | Visit 2 | n | Visit 3 | |
|---|---|---|---|---|---|---|
| SSD | 16 | 0.61 (0.54–0.89) | 15 | 0.83 (0.74–0.88) | 14 | 0.85 (0.77–0.96) |
| AHL | 22 | 0.48 (0.35–0.67) | 20 | 0.68 (0.55–0.79) | 19 | 0.74 (0.65–0.81) |
| Unilateral | 45 | 0.45 (0.36–0.56) | 43 | 0.67 (0.55–0.79) | 40 | 0.69 (0.50–0.74) |
| Visit | n | Total | Wilcoxon Signed-Rank Test (p-Values 2-Sided) | ||
|---|---|---|---|---|---|
| V1 vs. V2 | V1 vs. V3 | ||||
| SSD | 1 | 17 | 5.1 (4.2–6.4) | 0.034 | 0.020 * |
| 2 | 16 | 6.1 (4.8–6.8) | |||
| 3 | 16 | 6.6 (5.8–7.0) | |||
| AHL | 1 | 25 | 2.8 (1.2–2.5) | <0.001 * | <0.001 * |
| 2 | 24 | 4.5 (3.3–6.5) | |||
| 3 | 23 | 5.2 (4.0–6.5) | |||
| Unilateral | 1 | 42 | 2.3 (1.2–2.5) | <0.001 * | <0.001 * |
| 2 | 42 | 4.4 (2.8–5.6) | |||
| 3 | 38 | 4.8 (3.4–6.1) | |||
| Visit 1 | Visit 2 | Visit 3 | Wilcoxon Signed-Rank Test (p-Values 2-Sided) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Median (IQR) | n | Median (IQR) | n | Median (IQR) | V1 vs. V2 | V1 vs. V3 | ||
| SSD | Basic sound perception | 14 | 68.8 (60.6–82.5) | 11 | 80.0 (63.8–83.8) | 12 | 86.3 (68.8–90.6) | 0.046 | 0.016 * |
| Advanced sound perception | 11 | 92.5 (70.0–97.5) | 10 | 95.0 (80.0–97.5) | 9 | 97.5 (82.5–97.5) | 0.159 | 0.237 | |
| Advanced speech production | 10 | 76.3 (54.4–90.0) | 10 | 85.0 (70.0–93.1) | 7 | 80.0 (67.5–91.3) | 0.028 | 0.237 | |
| Self-esteem | 10 | 65.0 (58.8–74.4) | 9 | 72.5 (70.0–82.5) | 9 | 75.0 (72.5–82.5) | 0.107 | 0.051 | |
| Activity limitations | 15 | 82.5 (71.3–86.3) | 14 | 87.5 (80.6–95.0) | 14 | 93.8 (85.6–97.5) | 0.074 | 0.003 * | |
| Social interactions | 6 | 68.8 (58.8–76.9) | 6 | 75.0 (69.4–82.5) | 5 | 75.0 (72.5–77.5) | 0.042 | 0.068 | |
| AHL | Basic sound perception | 18 | 56.3 (35.6–66.9) | 18 | 65.0 (48.1–75.0) | 17 | 72.5 (67.5–77.5) | 0.005 * | 0.001 * |
| Advanced sound perception | 19 | 72.5 (55.0–83.8) | 17 | 82.5 (67.5–87.5) | 18 | 78.8 (75.0–86.9) | 0.006 * | 0.001 * | |
| Advanced speech production | 21 | 52.5 (35.0–75.0) | 19 | 70.0 (52.5–80.0) | 19 | 72.5 (62.5–85.0) | 0.014 * | 0.001 * | |
| Self-esteem | 19 | 60.0 (50.0–68.8) | 14 | 70.0 (64.4–74.4) | 17 | 72.5 (65.0–75.0) | 0.016 * | 0.010 * | |
| Activity limitations | 12 | 62.5 (45.6–75.6) | 12 | 75.0 (69.4–80.6) | 10 | 77.5 (71.9–79.4) | 0.009 * | 0.033 | |
| Social interactions | 8 | 46.3 (27.5–60.0) | 6 | 70.0 (63.8–72.5) | 8 | 65.0 (58.1–69.4) | 0.068 | 0.043 | |
| Unilateral | Basic sound perception | 42 | 35.0 (20.0–49.4) | 39 | 62.5 (48.8–81.3) | 36 | 71.3 (59.4–80.6) | <0.001 * | <0.001 * |
| Advanced sound perception | 35 | 70.0 (52.5–78.8) | 36 | 82.5 (68.8–92.5) | 30 | 83.8 (67.5–95.0) | 0.008 * | <0.001 * | |
| Advanced speech production | 40 | 32.5 (15.0–48.1) | 35 | 50.0 (38.8–61.3) | 34 | 57.5 (48.1–64.4) | <0.001 * | <0.001 * | |
| Self-esteem | 41 | 42.5 (30.0–52.5) | 35 | 65.0 (45.0–73.8) | 35 | 62.5 (55.0–77.5) | <0.001 * | <0.001 * | |
| Activity limitations | 29 | 40.0 (30.0–70.0) | 27 | 77.5 (55.0–86.3) | 25 | 77.5 (75.0–85.0) | <0.001 * | 0.001 * | |
| Social interactions | 20 | 47.5 (27.5–55.6) | 14 | 65.0 (52.5–73.1) | 17 | 67.5 (60.0–77.5) | 0.013 * | 0.002 * | |
| Hours per Day | |||||||
|---|---|---|---|---|---|---|---|
| n | 3–5 | 6–8 | 9–12 | 12–15 | >15 | ||
| AHL | Visit 2 | 19 | 0% | 0% | 36.8% | 52.6% | 10.6% |
| Visit 3 | 24 | 0% | 0% | 41.7% | 50.0% | 8.3% | |
| SSD | Visit 2 | 16 | 0% | 0% | 12.5% | 62.5% | 25.0% |
| Visit 3 | 16 | 6.3% | 6.3% | 25.0% | 50.0% | 12.5% | |
| Unilateral | Visit 2 | 49 | 0% | 6.1% | 32.7% | 44.9% | 16.3% |
| Visit 3 | 42 | 0% | 2.4% | 28.6% | 57.1% | 11.9% | |
References
- Contrera, K.J.; Betz, J.; Li, L.; Blake, C.R.; Sung, Y.K.; Choi, J.S.; Lin, F.R. Quality of life after intervention with a cochlear implant or hearing aid. Laryngoscope 2016, 126, 2110–2115. [Google Scholar] [CrossRef] [PubMed]
- Thompson, N.J.; Brown, K.D.; Dillon, M.T. Cochlear implantation for paediatric and adult cases of unilateral and asymmetric hearing loss. Curr. Opin. Otolaryngol. Head Neck Surg. 2022, 30, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Lassaletta, L.; Calvino, M.; Sanchez-Cuadrado, I.; Skarzynski, P.H.; Cywka, K.B.; Czajka, N.; Kutyba, J.; Tavora-Vieira, D.; van de Heyning, P.; Mertens, G.; et al. Using Generic and Disease-Specific Measures to Assess Quality of Life before and after 12 Months of Hearing Implant Use: A Prospective, Longitudinal, Multicenter, Observational Clinical Study. Int. J. Environ. Res. Public Health 2022, 19, 2503. [Google Scholar] [CrossRef]
- Weichbold, V.; Zelger, P.; Galvan, O.; Muigg, F. 5-Year Observation Period of Quality of Life After Cochlear Implantation. Otol. Neurotol. 2023, 44, e155–e159. [Google Scholar] [CrossRef]
- Horsman, J.; Furlong, W.; Feeny, D.; Torrance, G. The Health Utilities Index (HUI): Concepts, measurement properties and applications. Health Qual. Life Outcomes 2003, 1, 54. [Google Scholar] [CrossRef] [PubMed]
- Richardson, J.; Iezzi, A.; Khan, M.A.; Maxwell, A. Validity and reliability of the Assessment of Quality of Life (AQoL)-8D multi-attribute utility instrument. Patient 2014, 7, 85–96. [Google Scholar] [CrossRef]
- Dixon, P.R.; Shapiro, J.; Tomlinson, G.; Cottrell, J.; Lui, J.T.; Falk, L.; Chen, J.M. Health State Utility Values Associated with Cochlear Implants in Adults: A Systematic Review and Network Meta-Analysis. Ear Hear. 2023, 44, 244–253. [Google Scholar] [CrossRef]
- McRackan, T.R.; Hand, B.N.; Velozo, C.A.; Dubno, J.R. Validity and reliability of the Cochlear Implant Quality of Life (CIQOL)-35 Profile and CIQOL-10 Global instruments in comparison to legacy instruments. Ear Hear. 2021, 42, 896–908. [Google Scholar] [CrossRef]
- Andries, E.; Gilles, A.; Topsakal, V.; Vanderveken, O.M.; Van de Heyning, P.; Van Rompaey, V.; Mertens, G. Systematic Review of Quality of Life Assessments after Cochlear Implantation in Older Adults. Audiol. Neurootol. 2021, 26, 61–75. [Google Scholar] [CrossRef]
- Noble, W.; Jensen, N.S.; Naylor, G.; Bhullar, N.; Akeroyd, M.A. A short form of the Speech, Spatial and Qualities of Hearing scale suitable for clinical use: The SSQ12. Int. J. Audiol. 2013, 52, 409–412. [Google Scholar] [CrossRef]
- Hinderink, J.B.; Krabbe, P.F.; Van Den Broek, P. Development and application of a health-related quality-of-life instrument for adults with cochlear implants: The Nijmegen cochlear implant questionnaire. Otolaryngol. Head Neck Surg. 2000, 123, 756–765. [Google Scholar] [CrossRef]
- Cox, R.M.; Alexander, G.C. The abbreviated profile of hearing aid benefit. Ear Hear. 1995, 16, 176–186. [Google Scholar] [CrossRef] [PubMed]
- Kompis, M.; Pfiffner, F.; Krebs, M.; Caversaccio, M.D. Factors influencing the decision for Baha in unilateral deafness: The Bern benefit in single-sided deafness questionnaire. Adv. Otorhinolaryngol. 2011, 71, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Summerfield, A.Q.; Kitterick, P.T.; Goman, A.M. Development and Critical Evaluation of a Condition-Specific Preference-Based Measure Sensitive to Binaural Hearing in Adults: The York Binaural Hearing-Related Quality-of-Life System. Ear Hear. 2022, 43, 379–397. [Google Scholar] [CrossRef]
- Corrigendum. Otolaryngol. Head Neck Surg. 2017, 156, 391. [CrossRef]
- Peters, J.P.M.; van Heteren, J.A.A.; Wendrich, A.W.; van Zanten, G.A.; Grolman, W.; Stokroos, R.J.; Smit, A.L. Short-term outcomes of cochlear implantation for single-sided deafness compared to bone conduction devices and contralateral routing of sound hearing aids-Results of a Randomised controlled trial (CINGLE-trial). PLoS ONE 2021, 16, e0257447. [Google Scholar] [CrossRef]
- Borre, E.D.; Kaalund, K.; Frisco, N.; Zhang, G.; Ayer, A.; Kelly-Hedrick, M.; Reed, S.D.; Emmett, S.D.; Francis, H.; Tucci, D.L.; et al. The Impact of Hearing Loss and Its Treatment on Health-Related Quality of Life Utility: A Systematic Review with Meta-analysis. J. Gen. Intern. Med. 2023, 38, 456–479. [Google Scholar] [CrossRef]
- Dillon, M.T.; Kocharyan, A.; Daher, G.S.; Carlson, M.L.; Shapiro, W.H.; Snapp, H.A.; Firszt, J.B. American Cochlear Implant Alliance Task Force Guidelines for Clinical Assessment and Management of Adult Cochlear Implantation for Single-Sided Deafness. Ear Hear. 2022, 43, 1605–1619. [Google Scholar] [CrossRef]
- Capretta, N.R.; Moberly, A.C. Does quality of life depend on speech recognition performance for adult cochlear implant users? Laryngoscope 2016, 126, 699–706. [Google Scholar] [CrossRef]
- McRackan, T.R.; Hand, B.N.; Velozo, C.A.; Dubno, J.R. Association of Demographic and Hearing-Related Factors with Cochlear Implant-Related Quality of Life. JAMA Otolaryngol. Head Neck Surg. 2019, 145, 422–430. [Google Scholar] [CrossRef]
- Galvin, J.J., 3rd; Fu, Q.J.; Wilkinson, E.P.; Mills, D.; Hagan, S.C.; Lupo, J.E.; Padilla, M.; Shannon, R.V. Benefits of Cochlear Implantation for Single-Sided Deafness: Data from the House Clinic-University of Southern California-University of California, Los Angeles Clinical Trial. Ear Hear. 2019, 40, 766–781. [Google Scholar] [CrossRef]
- Skidmore, J.A.; Vasil, K.J.; He, S.; Moberly, A.C. Explaining Speech Recognition and Quality of Life Outcomes in Adult Cochlear Implant Users: Complementary Contributions of Demographic, Sensory, and Cognitive Factors. Otol. Neurotol. 2020, 41, e795–e803. [Google Scholar] [CrossRef]
- McRackan, T.R.; Hand, B.N.; Chidarala, S.; Dubno, J.R. Understanding Patient Expectations Before Implantation Using the Cochlear Implant Quality of Life-Expectations Instrument. JAMA Otolaryngol. Head Neck Surg. 2022, 148, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Illg, A.; Bräcker, T.; Batsoulis, C.; Opie, J.M.; Lesinski-Schiedat, A. CI decision making and expectations by older adults. Cochlear Implant. Int. 2022, 23, 139–147. [Google Scholar] [CrossRef]
- Prentiss, S.; Snapp, H.; Zwolan, T. Audiology Practices in the Preoperative Evaluation and Management of Adult Cochlear Implant Candidates. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.S.; Capretta, N.R.; Henning, S.C.; Feeney, L.; Pitt, M.A.; Moberly, A.C. Postoperative Rehabilitation Strategies Used by Adults with Cochlear Implants: A Pilot Study. Laryngoscope Investig. Otolaryngol. 2016, 1, 42–48. [Google Scholar] [CrossRef]
- Nijmeijer, H.G.B.; Groenewoud, H.M.M.; Mylanus, E.A.M.; Goedegebure, A.; Huinck, W.J.; van der Wilt, G.J. Impact of Expanding Eligibility Criteria for Cochlear Implantation Dynamic Modeling Study. Laryngoscope 2023, 133, 924–932. [Google Scholar] [CrossRef]
- Skarzynski, P.H.; Ciesla, K.; Lorens, A.; Wojcik, J.; Skarzynski, H. Cost-Utility Analysis of Bilateral Cochlear Implantation in Adults with Severe to Profound Sensorineural Hearing Loss in Poland. Otol. Neurotol. 2021, 42, 706–712. [Google Scholar] [CrossRef]
- Cutler, H.; Gumbie, M.; Olin, E.; Parkinson, B.; Bowman, R.; Quadri, H.; Mann, T. The cost-effectiveness of unilateral cochlear implants in UK adults. Eur. J. Health Econ. 2022, 23, 763–779. [Google Scholar] [CrossRef]
- Lindquist, N.R.; Holder, J.T.; Patro, A.; Cass, N.D.; Tawfik, K.O.; O’Malley, M.R.; Bennett, M.L.; Haynes, D.S.; Gifford, R.H.; Perkins, E.L. Cochlear Implants for Single-Sided Deafness: Quality of Life, Daily Usage, and Duration of Deafness. Laryngoscope 2023, 133, 2362–2370. [Google Scholar] [CrossRef]
- Andries, E.; Lorens, A.; Skarżyński, P.H.; Skarzynski, H.; Calvino, M.; Gavilan, J.; Lassaletta, L.; Tavora-Vieira, D.; Acharya, A.; Kurz, A.; et al. Evaluating the Revised Work Rehabilitation Questionnaire in Cochlear Implant Users Cochlear Implant Outcome Assessment Based on the International Classification of Functioning, Disability, and Health (ICF). Otol. Neurotol. 2022, 43, e571–e577. [Google Scholar] [CrossRef] [PubMed]
- Walker, E.A.; Spratford, M.; Moeller, M.P.; Oleson, J.; Ou, H.; Roush, P.; Jacobs, S. Predictors of hearing aid use time in children with mild-to-severe hearing loss. Lang. Speech Hear. Serv. Sch. 2013, 44, 73–88. [Google Scholar] [CrossRef] [PubMed]
- Walker, E.A.; McCreery, R.W.; Spratford, M.; Oleson, J.J.; Van Buren, J.; Bentler, R.; Roush, P.; Moeller, M.P. Trends and Predictors of Longitudinal Hearing Aid Use for Children Who Are Hard of Hearing. Ear Hear. 2015, 36 (Suppl. S1), 38s–47s. [Google Scholar] [CrossRef]




| n | Age at Time of Testing (Years) | n | Age at Implantation (Years) | n | Duration of Deafness in Implanted Ear (Years) | |
|---|---|---|---|---|---|---|
| SSD | 17 | 39.5 (16.4–66.4) | 16 | 39.9 (16.8–66.1) | 15 | 25.3 (9–67) |
| AHL | 26 | 64.6 (28.3–79.6) | 22 | 64.6 (29.0–78.4) | 17 | 18.8 (2–48) |
| Unilateral | 58 | 58.7 (24.1–84.7) | 52 | 60.3 (26.2–85.8) | 41 | 20.2 (2–63) |
| SSD | AHL | Unilateral | ||||
|---|---|---|---|---|---|---|
| Intervals | 1 v 2 | 1 v 3 | 1 v 2 | 1 v 3 | 1 v 2 | 1 v 3 |
| HUI-3 | Yes | Yes | Yes | Yes | Yes | Yes |
| SSQ12 (total score) | No | Yes | Yes | Yes | Yes | Yes |
| NCIQ | ||||||
| Basic sound perception | No | Yes | Yes | Yes | Yes | Yes |
| Advanced sound perception | No | No | Yes | Yes | Yes | Yes |
| Advanced speech production | No | No | Yes | Yes | Yes | Yes |
| Self-esteem | No | No | Yes | Yes | Yes | Yes |
| Activity limitations | No | Yes | Yes | No | Yes | Yes |
| Social interactions | No | No | No | No | Yes | Yes |
| Total | 5/16 | 13/16 | 16/16 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lassaletta, L.; Calvino, M.; Sanchez-Cuadrado, I.; Skarzynski, P.H.; Cywka, K.B.; Czajka, N.; Kutyba, J.; Tavora-Vieira, D.; Van de Heyning, P.; Mertens, G.; et al. QoL, CIs, QALYs, and Individualized Rehabilitation: The Clinical and Practical Benefits of Regularly Assessing the Quality of Life of Adult Cochlear Implant Recipients. Int. J. Environ. Res. Public Health 2023, 20, 6906. https://doi.org/10.3390/ijerph20206906
Lassaletta L, Calvino M, Sanchez-Cuadrado I, Skarzynski PH, Cywka KB, Czajka N, Kutyba J, Tavora-Vieira D, Van de Heyning P, Mertens G, et al. QoL, CIs, QALYs, and Individualized Rehabilitation: The Clinical and Practical Benefits of Regularly Assessing the Quality of Life of Adult Cochlear Implant Recipients. International Journal of Environmental Research and Public Health. 2023; 20(20):6906. https://doi.org/10.3390/ijerph20206906
Chicago/Turabian StyleLassaletta, Luis, Miryam Calvino, Isabel Sanchez-Cuadrado, Piotr Henryk Skarzynski, Katarzyna B. Cywka, Natalia Czajka, Justyna Kutyba, Dayse Tavora-Vieira, Paul Van de Heyning, Griet Mertens, and et al. 2023. "QoL, CIs, QALYs, and Individualized Rehabilitation: The Clinical and Practical Benefits of Regularly Assessing the Quality of Life of Adult Cochlear Implant Recipients" International Journal of Environmental Research and Public Health 20, no. 20: 6906. https://doi.org/10.3390/ijerph20206906